Acromioclavicular (AC) joint separation is one of the most common shoulder injuries seen in contact sports like football, rugby, and hockey. It occurs when the ligaments supporting the clavicle and shoulder blade are torn due to trauma. For athletes and active individuals, this injury can be both painful and visually deforming, often requiring expert surgical intervention.

Dr. Steven Struhl is a board-certified orthopedic surgeon with advanced fellowship training in sports medicine and over two decades of experience treating shoulder injuries. Practicing in New York City and Westchester, Dr. Struhl is internationally recognized for developing a patented surgical technique for AC joint reconstruction that addresses both vertical and medial instability—two key factors in long-term success.
Secondary support to the AC joint comes from the coracoclavicular ligament. This is a short strong ligament that connects the clavicle to the scapula and prevents downward movement of the scapula. It s has two separate components, the conoid, and the trapezoid.
What Is the AC Joint?
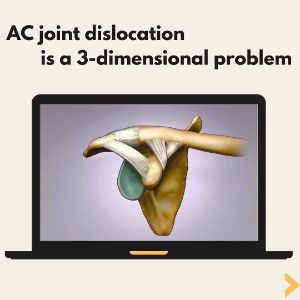
The acromioclavicular joint (AC joint) is where the collarbone (clavicle) meets the acromion, part of the shoulder blade (scapula). Though small, this joint plays a vital role in upper body movement and function—essentially suspending the arm from the axial skeleton. It’s stabilized by two major sets of ligaments:
- AC joint capsule – The first to be injured in most separations.
- Coracoclavicular (CC) ligaments – Including the conoid and trapezoid ligaments, these provide secondary stability and prevent downward displacement of the scapula.
Understanding AC Joint Separation
An AC joint separation typically results from a fall or direct blow to the top of the shoulder, especially in athletic or high-impact environments. When the AC and CC ligaments rupture, the shoulder blade drops away from the collarbone, creating a visible deformity—often mistaken for the clavicle being pushed upward.
However, Dr. Struhl’s research and surgical innovations have shown that the real problem is the scapula moving downward, not the clavicle moving upward. His technique focuses on lifting and securing the scapula back up to the clavicle, restoring proper anatomical alignment and function.
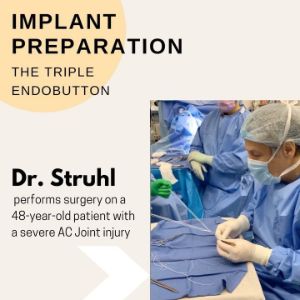
Dr. Struhl’s patented Triple Endobutton technique offers superior outcomes by addressing both vertical and horizontal instability, which is often missed in traditional procedures.
Signs and Symptoms of an AC Joint Injury
- A visible bump on the top of the shoulder
- Pain when lifting the arm or sleeping on the affected side
- Shoulder weakness or instability
- Clicking or grinding with movement
- Limited range of motion
If left untreated or improperly repaired, AC joint separations can lead to chronic pain, loss of strength, and early-onset arthritis in the shoulder.
Correct mechanism of injury
Incorrect mechanism of injury
Why Choose Dr. Steven Struhl?
- Board-Certified in Orthopedic Surgery and Sports Medicine
- Fellowship-Trained at Penn State in Sports Medicine
- Faculty at NYU Medical School
- Medical Consultant for the US Open Tennis Tournament
- Medical Director for Sportscare Physical Therapy (Brooklyn Nets)
- Inventor of a patented AC joint reconstruction technique
- Over 25 years of private orthopedic practice
Dr. Struhl has treated thousands of patients suffering from complex shoulder injuries and is frequently referred difficult cases from other surgeons. Patients come from across the country to consult with him on revision AC joint surgery.
FAQs About AC Joint Separation
How do I know if my shoulder bump is an AC joint separation?
A prominent bump after a shoulder impact could indicate a Grade 3 or higher AC joint separation. Clinical evaluation and imaging are necessary for a proper diagnosis.
Can AC joint injuries heal without surgery?
Mild separations (Grade 1–2) often heal with rest, physical therapy, and immobilization. More severe separations (Grade 3+) usually require surgical repair for full functional and aesthetic recovery.
What makes Dr. Struhl’s approach different?
Unlike standard procedures, Dr. Struhl’s patented method restores both vertical and medial stability—significantly reducing failure rates.
What is the recovery time after AC joint surgery?
Most patients return to non-contact activity within 3 months and full contact sports by 5–6 months post-op, depending on their specific case and rehab compliance.
Is this procedure covered by insurance?
Yes. Most insurance plans cover AC joint separation surgery when medically necessary. Our office staff can assist with benefit verification.
Schedule Your Consultation
If you’ve suffered an AC joint injury, don’t risk chronic instability or surgical failure. Schedule a consultation with Dr. Steven Struhl in NYC or Westchester and learn more about your options for lasting recovery.
📞 NYC Office: (212) 207-1990
📞 Westchester Office: (914) 328-4111
Clinical Demonstration of mechanism of injury
A complete AC joint separation creates a deformity. The protruding bump is the edge of the clavicle. While it seems obvious that the problem is the protruding bone that needs to be pushed back down, the solution actually requires just the opposite! The scapula needs to be pushed back up to meet the clavicle and supported there with adequate fixation. The video demonstrates that reducing the joint requires pushing the scapula “up” to the clavicle, not the other way around:
How understanding the mechanism of injury leads to successful surgery with the Triple Endobutton Technique.
The importance medial instability that occurs from an AC joint separation
After an AC joint dislocation not only does the scapula drop down and away from the clavicle but it also results in significant medial instability. This video shows how this instability leads to symptoms and how the Triple Endobutton uniquely addresses it leading to successful surgical outcomes.
Closed-Loop Double Cortical Button Technique for AC Joint Dislocations
Dr. Struhl’s Closed-Loop Double Cortical Button Technique (often referred to as the Triple Endobutton procedure) is a cutting-edge, minimally invasive solution. This technique provides:
- Strong, anatomic fixation
- Reduced recovery times
- Improved cosmetic outcomes
- Durable long-term stability
Most importantly, it reflects a deep understanding of the true mechanism of injury, correcting the common misconceptions that lead to surgical failure.